On this page
- Introduction to Quantitative Nuclear Medicine
- Planar whole body distributions
- Use of Standards in Emission Tomography
- Partial Volume Effect in Emission Tomography
- Quantitative Assessment in Emission Tomography
- Estimation of Activity in Emission Tomography
- Evaluation of Image Quality in Emission Tomography
Introduction to Quantitative Nuclear Medicine
Quantitative tasks involve extracting a numerical value or values from data obtained in a nuclear medicine procedure. Over the past 15 years, methods have been developed to accurately quantify nuclear medicine images. Nuclear medicine images can be used for detection tasks, such as identifying perfusion defects, or quantitative tasks, such as estimating ejection fraction, standardized uptake values (SUVs) or organ absorbed dose. Obtaining images suitable for quantitative tasks often requires additional processing compared with those used for visual interpretation. This additional processing often results in improved resolution and contrast and reduced artefacts. These improvements in the image will often, but not always, translate directly to improved performance on detection tasks. For example, the development of attenuation correction methods for cardiac single photon emission computed tomography (SPECT) has improved detection of myocardial perfusion defects, while at the same time providing images which are quantitatively more accurate.
The topic of quantitative nuclear medicine is discussed in a broad range of publications. However, the IAEA Human Health Report No.9 “Quantitative Nuclear Medicine Imaging: Concepts, Requirements and Methods” provides a well-structured and detailed report to the matter. In addition, the IAEA book on Nuclear Medicine Physics provides a comprehensive overview to the field of nuclear medicine.
Planar whole body distributions
Planar imaging is still used clinically in nuclear medicine, although tomographic imaging (single photon emission computed tomography (SPECT) and positron emission tomography (PET)) are becoming more established. Planar whole-body imaging is almost always carried out by translating the patient and bed in the z-direction between opposed heads of a dual head standard scintillation camera. The cameras are typically positioned anterior and posterior relative to the patient
One approach to planar imaging is to perform conjugate counting with the geometric mean, which consists of acquiring data from opposite views and combining them into a single dataset. Figure 1 shows an imaging object with uniform attenuation viewed by two gamma detectors placed in opposite directions. A point source in the object has the attenuation depth d1 and d2 to detectors 1 and 2, respectively. This approach is only exact for point-sources, but corrections can be made for extended sources. The geometric mean using conjugate views is a popular quantification method for planar imaging.
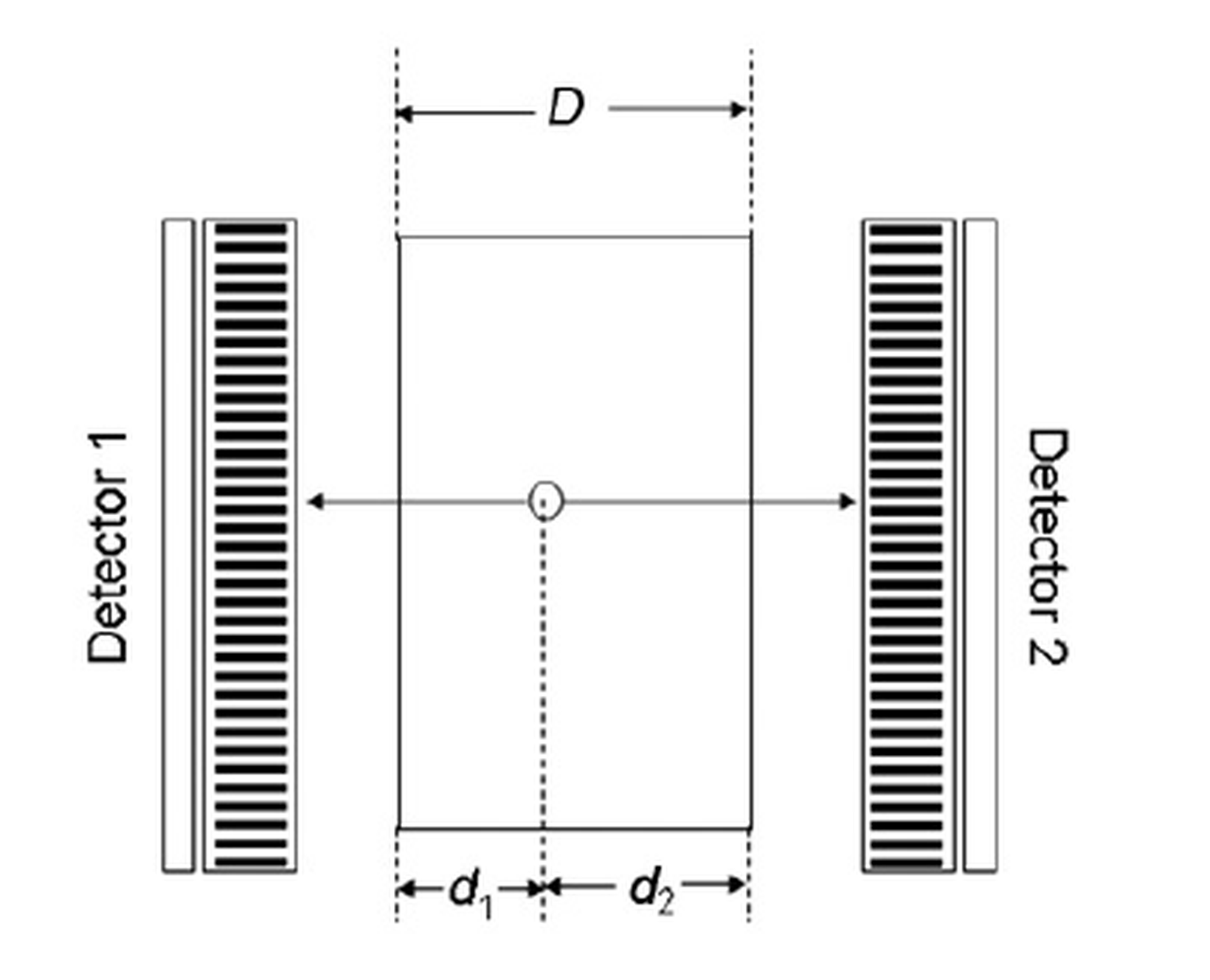
<p>Figure 1: Illustration of conjugate viewing with the geometric mean for attenuation compensation (Source: IAEA Nuclear Medicine Physics, p.609)</p>
The thickness of the patient, expressed as D in the equations above, can be measured either by determining the thickness of the patient at various points of the body manually or a separate transmission study. By mounting a photon flood source on the opposite side of the camera relative to the patient, the transmission of the photons can be measured. This procedure includes two measurements: one with and one without the patient. The pixel by pixel ratio of the counts with the patient present divided by the counts with the patient absent gives the attenuation factor. Non-target activity can be defined as both over- and underlying activity from other organs and tissues but also the blood activity within the organ itself. A proper ROI (region of interest) location correcting for the non-target activity is therefore of great importance. The contribution from activity in the overlap region can be determined from the data in the non-overlapped regions. The background activity is determined from the activity per pixel in a representative ROI and the fraction of patient thickness occupied by the particular organ.
The subject of planar whole-body imaging is elaborately discussed in the IAEA Human Health Report No.9 “Quantitative Nuclear Medicine Imaging: Concepts, Requirements and Methods” and the IAEA book on Nuclear Medicine Physics. The latter also provides a comprehensive overview to the topic of Nuclear Medicine in general.
Use of Standards in Emission Tomography
Nowadays, Single Photon Emission Tomography (SPECT) and Positron Emission Tomography (PET) are widely used and accepted methods for diagnosing and treating diseases. They are helpful in cancer care for finding tumors, deciding treatment stages, and checking how well treatments are working. They are also used in heart care to check heart health and blood flow, and in brain care to study blood flow and brain cell connections.
Important principles
PET operates on the principle of detecting two photons that are emitted 180o apart from each other, resulting from the annihilation of a positron and an electron. Utilizing suitable radiation detectors and coincidence electronic circuits, these two photons are identified concurrently within a restricted time frame. In contrast, SPECT systems employ a gamma camera detector that can rotate around the subject to generate projection images from various angles, supplying the necessary data to reconstruct a three-dimensional representation of activity.
When performing quantification from projections in the clinic, it can be helpful to image a standard activity (known measured activity) along with the patient. The standard (usually a small probe of the radiotracer) provides a conversion between radioactivity concentration (MBq/mL) and counts in the projections. It should be noted that the use of standards does not guarantee accurate absolute quantification because the standard activity is not affected by scatter, attenuation and partial volume effects in the same way as the activity distribution in the patient.
The subject of Emission Tomography is covered in a broad range of literature as it is established as an integral part of the field of nuclear medicine. The IAEA publications Human Health Series No.1 “Quality Assurance for PET and PET/CT Systems” and Human Health Series No.36 “SPECT/CT Atlas of Quality Control and Image Artefacts” provide a very detailed description of the imaging techniques and also contain guidelines for quality control. The IAEA reference book Nuclear Medicine Physics, in addition, gives a comprehensive overview of the topic of nuclear medicine in general.
Partial Volume Effect in Emission Tomography
Single Photon Emission Tomography (SPECT) and Positron Emission Tomography (PET) are important imaging methods in nuclear medicine and help find cancer cells early. In a perfect situation, the activity strength in a certain area of a reconstructed image should match the real activity level in that area. However, the partial volume effect (PVE) greatly influences the measurement because of the size of the object being studied.
Important principles
The PVE includes two different phenomena: One is the image blurring effect caused by the finite spatial resolution where the blurring results in spill-over between regions. The image of a hot region (i.e., tumour with radiotracer uptake) appears larger and dimmer. The other PVE phenomenon is the tissue fraction effect caused by the fact that the boundaries of certain data points do not match the underlying activity distribution. The net PVE effect is the reduced contrast between the object and the surrounding areas, as well as the reduced absolute uptake in a hot region. For tumour imaging, the PVE can affect both the tumour’s apparent uptake and tumour apparent size. The PVE correction is dependent on the size and shape of the region, the activity distribution in the surrounding background, image spatial resolution, pixel size and how uptake value is measured. The PVE correction is complicated by the fact that not only activity from inside the region spills out but also activity from outside the region spills in. As these two activity dependent flows are not usually balanced, it is difficult to predict the overall PVE effect.
The ratio of the apparent concentration to true concentration is called the recovery coefficient (RC). If the spatial resolution of the system can be characterized at the location where the object of interest is (this is usually the case in both SPECT and PET as the dependence of spatial resolution on location is known), and if the size and shape of a region are known the RC can be pre-calculated and then applied to the measured concentration value in the region. As the RC depends on the activity concentration in the region and in the surrounding background, the RC will be different if the surrounding background is also hot.
The subject of quantification in emission tomography is covered in the IAEA reference book Nuclear Medicine Physics. The IAEA publications Human Health Series No.1 “Quality Assurance for PET and PET/CT Systems” and No.36 “SPECT/CT Atlas of Quality Control and Image Artefacts” discuss the principles of SPECT and PET in depth and provide proper information on quality control.
Quantitative Assessment in Emission Tomography
Single Photon Emission Tomography (SPECT) and Positron Emission Tomography (PET) are important imaging methods in nuclear medicine and help find cancer cells early. We can analyze the images we get by comparing the target area to the background, looking at the amount of radiotracer, or by studying the change in specific characteristics over time.
Important principles
The target to background contrast is the ratio between the concentration within the target region and the concentration within the surrounding background.
The radiotracer concentration (Bq/mL) is the amount of radioactivity per unit volume within a defined region of interest (ROI). The standardized uptake value (SUV) is the radiotracer concentration normalized by injected dose and patient weight, and is mainly used to assess
tumour glucose utilization for fluorodeoxyglucose (FDG) PET. The primary use of the SUV is to quantify activity in an ROI independent of administered activity and patient weight.
Dynamic imaging consists of acquiring data as a series of time frames that capture the time–activity curve in each data point over time, making it possible to quantify tracer kinetics in vivo. With an understanding of the underlying physiological factors that control the tissue radioactivity levels, mathematical models, known as kinetic models, can be constructed with one or more parameters that describe the distribution of radiotracers as a function of time in the body and fit the time-activity curves in each data point in the organ of interest. Kinetic models used in Nuclear Medicine are based on compartments within a volume or space within which the radiotracer becomes uniformly distributed almost instantly, i.e., contains no significant concentration gradients. In other words, compartmental modelling describes systems that vary in time but not in space. More complicated kinetic models that include spatial gradients are generally not applicable to nuclear medicine because of limited spatial resolution.
The subject of quantification in emission tomography is covered in the IAEA book on Nuclear Medicine Physics. The IAEA publications Human Health Series No.1 “Quality Assurance for PET and PET/CT Systems” and No.36 “SPECT/CT Atlas of Quality Control and Image Artefacts” discuss the principles of SPECT and PET in depth and provide proper information to quality control.
Estimation of Activity in Emission Tomography
The measurement and estimation of radioactivity is fundamental in all Nuclear Medicine applications including Single Photon Emission Tomography (SPECT) and Positron Emission Tomography (PET). In order to correctly estimate the activity in a patient, uncertainties and deviations need to be quantified. Bias, precision and accuracy are three important statistical concepts for this purpose.
Important principles
Activity is a measure of the number of nuclear transformations occurring per unit of time. According to the International System of Units (SI), the unit for activity is the becquerel (Bq), defined as one transition per second, and is measured in reciprocal seconds (s–1). The goal of quantitative nuclear medicine is to determine the absolute activity in a given volume by external measurement of the radiation emitted by the patient. In order to quantify occurring uncertainties in the measurements and therefore enable estimation of the actual activity statistical concepts like bias, precision and accuracy have proven to be very useful.
Bias is the difference between a population mean of the measurements or test results and an accepted reference or true value. The Bias is mainly due to faulty measuring devices or procedures.
Precision, defined as the deviation between repeated measurements, can be quantified by the variance. It is important to note that the calculation of precision does not require knowledge of the true value. Therefore, precision alone cannot be used to evaluate the performance of a measurement.
Bias and precision can be combined to assess the performance of a measurement. Less biased and more precise measurements yield more accurate estimations. Thus, accuracy is defined as the overall difference between the measured value and the true value and can be quantified by the mean square error (MSE). To have the same scale as the mean value, precision is also quantified by standard deviation, defined as the square root of variance and accuracy is also quantified as the square root of MSE.
The subject of estimation of activity in nuclear physics is covered in the IAEA book on Nuclear Medicine Physics, and the IAEA Human Health Report No.9 “Quantitative Nuclear Medicine Imaging: Concepts. Requirements and Methods” provides additional information on the topic of quantitative nuclear medicine in general.
Evaluation of Image Quality in Emission Tomography
Image quality is a concept that has no objective definition and often is a matter of the observer’s subjective judgement. A good surrogate for image quality is image utility, thus, in the field of Nuclear Medicine, image quality correlates with the ability to detect differences in the uptake of a radiopharmaceutical in a lesion and its surroundings. Hence, an image of high quality is one that can reproduce this contrast in order to secure a correct diagnosis.
Important principles
Image quality is dependent on the inherent properties of the imaging device (i.e., spatial resolution) and the patient and organ localization (i.e., the size of the patient).
In order to evaluate image quality, measures of quantitative accuracy, precision and root MSE are very useful when first assessing a new system or a quantification method. However, for more rigorous evaluation or for optimization of image quality it is recommended to carry out an objective assessment of image quality based on detection or quantification tasks. Performance metrics for task-based estimation or detection tasks can be viewed as measures of image utility, which are the most clinically relevant bases on which to evaluate or optimize imaging systems. The most conclusive assessment of image quality is based on human-observer studies. However, such studies are not routinely performed clinically because they are time and resource consuming. Instead, a numerical observer is often used.
Evaluation and optimization of image quality has received a lot of attention recently and is a topic covered in a lot of publications. The IAEA handbook “Nuclear Medicine Physics” provides comprehensive information about the subject of imaging in Nuclear Medicine. Additional information on the topic can also be found in the IAEA Human Health Report No.9 “Quantitative Nuclear Medicine Imaging: Concepts, Requirements and Methods”.